

What is Hypertrophic Pyloric Stenosis?
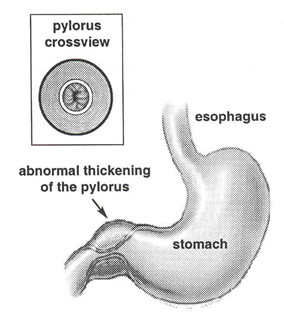
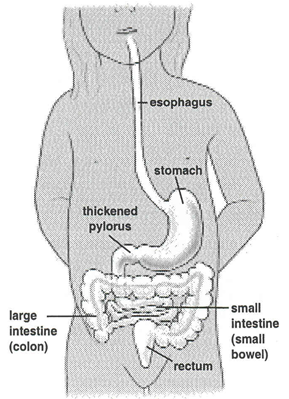
Hypertrophic pyloric stenosis (HPS) is an abnormal thickening of the pylorus muscle through which food and other stomach contents pass into the small intestine.
The thickened pyloric muscle causes a narrowing of the pyloric channel. As a result, breastmilk or infant formula feedings cannot pass out of the stomach into the small intestine.
What are the symptoms of HPS?
Because infants with pyloric stenosis are unable to tolerate their feedings, they may have the following symptoms:
- Frequent episodes of projectile vomiting (forceful vomiting) within 30 to 60 minutes after feedings
- Small stools
- Dehydration
- Weight loss
- Irritability
- Hunger after feedings
How common is HPS?
HPS affects three out of every 1,000 babies born. It is more likely to affect full-term, first-born male infants and affects female infants less frequently. HPS is more common in Caucasian infants, especially those of European descent.
About 15 percent of infants born with HPS have a family history of the condition.
An infant is three times more likely to develop HPS if the mother had the disease as an infant, as compared to the father.
When does HPS occur?
The symptoms of HPS usually occur between the third and sixth week of life.
How is HPS diagnosed?
HPS is diagnosed after evaluating your baby’s feeding habits and performing a physical examination. Your health care provider will ask you several questions about your baby’s feeding habits and will then examine your baby.
During the physical exam, the health care provider may be able to feel an olive-sized lump in your baby’s abdomen, which is the thickened pyloric muscle. If the thickened pylorus is felt, no further studies are needed.
If the thickened pylorus cannot be felt, an abdominal ultrasound may be done. During the examination, a probe is gently applied against the abdomen. The probe transmits sound waves through the body tissues, receives the echoes and transforms them into diagnostic images. Often the enlarged pyloric muscle can be seen on the ultrasound images.
Sometimes an upper gastrointestinal series must be done if the physical exam and abdominal ultrasound do not reveal any abnormalities. This test requires that your baby drink a special liquid.
This liquid can be seen on an X-ray as it travels through the stomach and small intestine. The pediatric radiologist will be viewing the X-ray while your baby drinks the liquid to determine whether or not the liquid is able to move out of the stomach through the pylorus.
How is HPS treated?
After accurately diagnosing HPS from the physical exam, ultrasound or gastrointestinal studies, surgery must be done to correct the condition.
Because infants with HPS are often dehydrated from extended vomiting, proper replacement of fluids is necessary before surgery can be performed. Blood tests can help detect dehydration. Sometimes, delivering fluids intravenously (through a vein in the arm) is necessary.
Before the surgery
Your baby will not be allowed to have any milk or formula for 6 hours before surgery to reduce the risk of vomiting and aspiration while under anesthesia.
During the surgery
- An anesthesiologist (a doctor who specializes in sedation and pain relief) gives your child general anesthesia, which induces sleep.
- A small incision is made on the left side of the abdomen, higher than the umbilicus (belly button).
- The surgeon then performs a “pyloromyotomy”, which involves making an incision in the thickened pylorus to allow food to move out of the stomach into the intestines properly. This procedure generally takes less than an hour to complete.
After the surgery
The usual length of stay after surgery is 24 to 36 hours. Several hours after surgery, your child will be able to eat again. Oral (by mouth) feedings are started very slowly, in very small amounts. The volume and concentration of the formula will be increased as your baby is able to tolerate the feeding.
If you breastfeed your baby, breast milk must be given to your baby through a bottle for the first few feedings so that it can be accurately measured.
Sometimes, babies will still vomit after surgery, but this does not mean that they have pyloric stenosis again. Other reasons why your baby might vomit after surgery include the anesthesia, advancing feedings too quickly and being inadequately burped after feedings.
If your baby continues to vomit for a prolonged period, your baby may need more tests. Before your baby is discharged from the hospital, the problem will be corrected.
Caring for your child after surgery
Your child will be eating normally by the time you go home. Usually, non-narcotic pain medication (such as Tylenol) is all that is needed to control minimal postoperative pain.
You may give your child a sponge bath the day after surgery. You may bathe your child in the tub 3 days after surgery.
The small piece of tape covering the incision (called a Steri-Strip) will gradually fall off on its own. Do not pull this tape off yourself. If the Steri-Strip has not fallen off by the time of your follow-up appointment, your health care provider will remove it for you.
When to call your child’s provider
You may notice some minor swelling around the incision; this is normal. However, call you health care provider if your child has a fever, excessive swelling, redness or drainage from incision, bleeding or increasing pain.
Follow-up appointment
A follow-up outpatient visit will be scheduled 7 to 10 days after your child’s surgery. Your child’s health care provider will examine the wound site and evaluate your child’s recovery.
[microinv id=microinv_1420922304]
Leave a reply
{kind=link}