

What are Pectus Excavatum and Pectus Carinatum?
Pectus excavatum is a common abnormality of the breastbone (sternum) in which the sternum is sunken, giving it the appearance of a cup or bowl on the front of the chest. It occurs in about one out of every 5,000 children. It is more common in boys than it is in girls.

Pectus carinatum is a variant of the breastbone defect. In this condition, the sternum protrudes in a “pigeon breast” deformity. This is much less common than pectus excavatum.

What are the symptoms of pectus excavatum and carinatum?
The symptoms of pectus excavatum and carinatum can vary; however, often the child has no symptoms. Children might complain of shortness of breath or pain with exertion. There might be symptoms of asthma, especially with exertion. In addition, the parents, caregivers, or coaches might notice that the child has a problem keeping up with peers during practices and active sporting events.
How are pectus excavatum and carinatum diagnosed?
The pectus deformity is diagnosed by visual inspection. Quite often, the defect does not become noticeable until the child has a significant growth spurt. In a small percentage, the defect will be noticeable at birth.
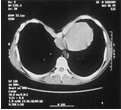
To prove medical necessity for the insurance companies to approve surgical treatment, the following diagnostic tests are ordered:
.
- Chest CT scan
- Pulmonary function tests (PFTs)
- Echocardiography
- Photography of chest
.
The results of these studies determine the severity of the deformity.
How are pectus excavatum and carinatum treated?
The treatment for pectus excavatum is to elevate the sternum into a normal position and contour, and to allow the cartilage that anchors the sternum to the ribs to reform in a more normal shape.
Pectus carinatum does not lend itself to a minimally invasive surgical approach. This repair requires an open incision and removal of the malformed cartilage. This allows for repositioning of the breastbone. The cartilage eventually re-grows, which anchors the breastbone in more normal position.
Nuss Minimally Invasive vs. Open Costosternoplasty
The standard repair procedure is costosternoplasty. During this procedure, an incision is made on the chest, the pectoris muscles are elevated, and the cartilage on both sides of the sternum are removed to allow elevation of the sternum.

A most recent development in repair is the Nuss minimally invasive procedure. This procedure is done with the assistance of a video scope placed in the chest. A bar is passed behind the breastbone, which allows for elevation of the breastbone into the adequate position.

What happens after surgery?
After the surgery, your child will be in the hospital 3-5 days. An epidural catheter that is placed prior to the surgery will help manage any postoperative discomfort.
When will my child be discharged?
Once your child’s pain is managed with oral pain medicine and he or she is back on a regular diet, your child will be ready for discharge.
What can I expect after discharge?
After discharge there will be progressive activity. Those children with bars in place will have rapid progression of their activities and may begin weight lifting at about six weeks after surgery. The bar remains in place for about two years after the procedure. An outpatient procedure is required for removal.
When should I call my child’s surgeon?
Call your child’s doctor if you notice any of these symptoms: fever, shortness of breath, excessive pain, and redness or drainage from the incisions.
Follow-up office appointments
Five follow-up appointments will be made at approximately two-week intervals after repair, until which time regular activity will be re-instituted. Follow-up appointments will remain at 6-12 month periods for several years after the repair to ensure stability.
[microinv id=microinv_1420922607]
Leave a reply
{kind=link}