

What is Esophageal Atresia?
Esophageal atresia (EA) is a congenital (present at birth) abnormality of the esophagus in which the upper portion of the esophagus ends in a blind pouch and is disconnected from the lower portion of the esophagus. In the most common form of esophageal atresia, which occurs in more than 85 percent of all cases, the lower esophagus has an abnormal connection to the trachea, called a tracheoesophageal fistula (TEF). There is a normal connection between the lower esophagus and the stomach (Figure 1).
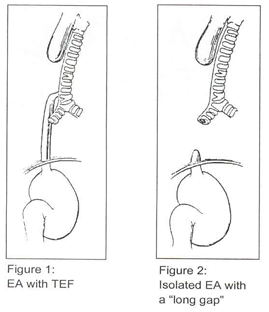
Less common variations include isolated EA without TEF, which occurs about 7 percent of the time. This is almost always associated with a long gap between the ends of the upper and lower esophageal pouches (Figure 2). Other, less common variations can also occur.
How common is esophageal atresia?
EA and TEF occur in 1 in 3,000 births, making it one of the more common correctable congenital anomalies.
What are the symptoms of esophageal atresia?
The first symptom is usually excessive drooling of saliva, which cannot be swallowed. When the baby is fed, choking and coughing usually occur, and the feeding is regurgitated. Babies will sometimes become cyanotic and can develop respiratory distress.
How is esophageal atresia diagnosed?
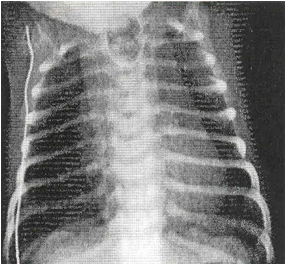
EA is initially suspected when difficulty swallowing occurs. Attempts are then made to pass a tube through the nose, down the esophagus and into the stomach (called a “nasogastric tube”). In EA, the tube cannot pass into the stomach and will coil in the blind upper pouch, producing an X-ray that is diagnositic for EA.
If no gas is visible in the abdomen on X-ray, a TEF is not present , and long gap isolated esophageal atresia is diagnosed. Although the majority of EA cases are diagnosed after birth, prenatal fetal ultrasound that shows polyhydramnios (excess fluid in the uterus) combined with failure to demonstrate the fetal stomach, suggests EA.
Is esophageal atresia associated with other anomalies?
Esophageal atresia can be associated with abnormalitites in other organ systems. EA is part of a condition called the VACTERL syndrome:
- V – vertebral anomalies
- A – anorectal anomalies
- C – cardiac anomalies
- TE – esophageal atresia and TEF
- R – renal anomalies
- L – limb anomalies
Your baby will receive a complete evaluation of all these organ systems during his or her stay in the hospital.
How is esophageal atresia treated?
The treatment of esophageal atresia is surgical. In the most common form of EA (EA with TEF), your baby will have surgery within several days of birth.
What happens during the surgery?
Your baby will be placed under general anesthesia and will be asleep for the duration of the procedure. Your baby will be placed on his or her side, and an incision will be made on the chest wall (thoractomy) in the lower axilla (armpit) at about the lower edge of the breast.
The surgeon then enters the chest between the ribs, and the lung is gently held aside. The surgeon will carefully disconnect the lower esophagus from the trachea and join it to the upper esophagus with a series of sutures. These will dissolve later, after the esophagus is healed. A chest tube is placed to allow fluid to drain from the surgical field and will exit the baby’s skin. Sometimes, a temporary feeding tube is placed into the stomach and will exit from the abdominal wall. The surgery usually takes about three hours.
What happens after surgery?
After surgery, your baby will return to the Neonatal Intensive Care Unit (NICU). Usually, the breathing tube will stay in for one or two days after the surgery and will then be removed. Your baby will not feed by mouth until five to seven days after surgery, when a swallowing study will be performed. When this verifies the esophagus has healed properly, your baby will begin feeding. Feeding will start very slowly and will be advanced over several days until normal feedings are established. The chest tube is usually removed a day after feeding begins.
When will my baby be discharged?
When you baby is tolerating full feedings by mouth, he or she will be discharged from the hospital.
What should I expect after discharge?
At home, you can feed your baby normally. Do not be alarmed if your baby takes smaller volumes of feedings at first. This is normal and will improve with time. Your surgeon will arrange for follow-up visits to monitor your baby’s progress.
What if my baby has long gap isolated EA?
While the surgical treatment of the ost common form of EA (EA with TEF) is well defined, the treatment of less common forms of EA – notably long gap isolated EA – is somewhat variable. Long gap EA is more difficult to manage because the esophagus usually cannot be immediately repaired due to excessive distance between the two ends of the esophagus.
Although some centers have advocated “replacing” the esophagus with stomach or colon conduits, we make every attempt to reconnect the native esophagus to itself. We do this by “stretching” the upper esophageal pouch over a period of six to eight weeks, during which time your baby will need to stay in the hospital. A soft tube or “dilator” is inserted by mouth into the upper esophageal pouch one to two times per day to lengthen the upper esophageal poucy. This is not painful. In most cases, we have been able to decrease the distance between the two ends of the esophagus so they can be put back together. In our experience, restoring the native esophagus leads to the best possible swallowing function after surgery.
[microinv id=microinv_1420923172]
Leave a reply
{kind=link}