

What is Gastroesophageal Reflux?
Gastroesophageal reflux is a digestive disorder that affects the lower esophageal sphincter (the muscular ring connecting the esophagus with the stomach). The sphincter normally prevents food from moving out of the stomach and back up into the esophagus.
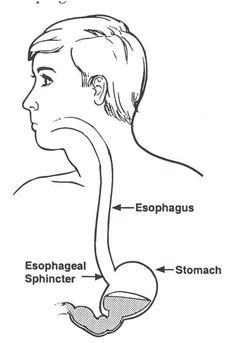
When a person has gastroesophageal reflux, the sphincter muscle becomes weak or fails to close tightly, causing food and stomach acids to flow back (reflux) into the esophagus. The lining of the esophagus can become inflamed or irritated from these acids, and cause a burning chest pain and sometimes a sour taste or cough.
Reflux also can cause aspiration pneumonia or failure to grow. In children with neurological disorders, reflux is made worse by failure of the stomach to empty properly.
What is the treatment for gastroesophageal reflux?
Management of reflux can sometimes be achieved before surgery is necessary. Techniques that often help include:
- Feeding the child smaller, more frequent meals
- Positioning the child upright for one hour after a feeding
- Giving medications as prescribed by your child’s health care provider
.
When is surgery necessary?
Children with severe, chronic esophageal reflux may need surgery to correct the problem if their symptoms are not relieved through other medical treatments. If left untreated, chronic gastroesophageal reflux can cause complications such as aspiration pneumonia, bleeding or scarring of the esophagus and failure to thrive.
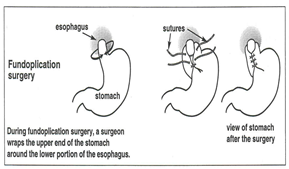
A Nissen fundoplication is a surgical procedure that corrects gastroesophageal reflux by creating an improved valve mechanism at the bottom of the esophagus.
Sometimes, a gastric emptying study (GES) is performed to determine if the stomach is emptying properly or if it is delayed. If the stomach is not emptying properly, reflux may occur.
If delayed gastric emptying is found, a surgical procedure called a pylorplasty may be necessary. A pyloroplasty widens the canal between the stomach and the small intestine in order to speed up the movement of gastric contents and allow the stomach to empty normally.
Before the surgery
Your child’s health care providers will reduce your child’s intake of food and fluids before the surgery to reduce the risk of vomiting and aspiration while under anesthesia. Here are some guidelines:
- Your child should not be given solid food for 8 hours before the surgery.
- Your child may have milk or formula for up to 6 hours before surgery.
- Your child may have breast milk or clear liquids (which include water, apple juice, popsicles and soup broth) up to 3 hours before surgery.
- Three hours before the surgery, you child should have nothing by mouth or feeding tube.
.
During the surgery
.
- An anesthesiologist (a physician who specializes in sedation and pain relief) gives your child general anesthesia, which induces sleep.
- A horizontal incision (cut) from 5 to 10 cm is made on the left side of the abdomen.
- The surgeon wraps the upper part of the stomach (called the fundus) around the lower portion of the esophagus. This creates a permanently tight sphincter so that food will not reflux back into the esophagus.
- The surgery takes about 2 hours.
.
After the surgery
Your child may be in the hospital for 3 to 5 days after the surgery. Occasionally, a nasogastric tube will be placed through your child’s nose and into the stomach. If your child requires supplemental feedings, a tube will be placed directly into the stomach. These tubes remove gas or gastric secretions directly from the stomach in order to keep the pressure low in the stomach and protect the incision and sutures.
An intravenous (IV) line will be placed in your child’s arm or hand to deliver fluids until feedings are resumed. When bowel sounds return and your child begins to pass gas, we will gradually advance your child’s diet. This process usually takes a few days.
Pain medications will be given to your child as needed. After your child has started eating again, has had a bowel movement and is feeling more comfortable, he or she will be discharged from the hospital.
Caring for your child after surgery
Usually, your child will be able to resume light activity within a few days of surgery. Heavy lifting and strenuous activity should be avoided for 3 weeks after surgery. Generally, children can return to school within a few days after being discharged from the hospital. You may give your child a sponge bath the day after surgery. Tub baths are permitted 4 to 5 days after surgery.
The small pieces of tape covering your child’s incisions (called steri-strips) will gradually fall off on their own. Do not pull these strips off yourself. If the strips do not fall off on their own, your health care provider will remove them at your child’s follow-up appointment.
When to call your child’s health care provider
You may notice some minor swelling around the incision; this is normal. However, call your health care provider if your child has:
- A fever
- Excessive swelling
- Redness
- Bleeding
- Increasing pain
.
Follow-up appointment
A follow-up appointment will be scheduled from 7 to 10 days after your child’s surgery. Your child’s health care provider will assess the wound site and his or her recovery.
[microinv id=microinv_1420922736]
Leave a reply
{kind=link}